By Cort Johnson on August 6, 201324 Comments
Small Fiber Nerve Study Suggests New Era in Fibromyalgia (and Perhaps Chronic Fatigue Syndrome) Could Be At Hand
I think that this is such big news because it gives proof that this disease is not in peoples heads. I really hope that we can get the word out to patients and even more importantly… the primary care docs and rheumatologists. These studies are “game changers” because they make an incredibly elusive disease tangible and “real”. –Dr. Mark Sivieri
My eyes widened as I looked over at the symptoms this new possible cause of FM/ME/CFS could produce. There it was: burning pain–one of my ‘favorite’ symptoms. More than any other symptom ‘burning pain’ after exercise has been a hallmark for me since I came down with chronic fatigue syndrome over thirty years ago.
Have researchers found a missing piece to fibromyalgia and chronic fatigue syndrome?
There were many more pain symptoms–shooting pain, allodynia, and hyperesthesia, plus many autonomic nervous symptoms. Some ME/CFS/FM docs were finding orthostatic intolerance as well. In fact, one doctor suggested this new finding could, depending on where it was found, possibly account for ALL the symptoms of ME/CFS/FM.
Dr. Teitelbaum had just told me he, Dr. Sivieri, and other physicians in an ME/CFS/FM working group were exploring a new avenue he hoped might particularly help the really hard to treat patients. He and Dr. Sivieri both stressed their results were very preliminary, but both were excited about a possible new cause for fibromyalgia and chronic fatigue syndrome. It is called ‘small fiber neuropathy’ (SFN).
Small Fiber Neuropathy (SFN)
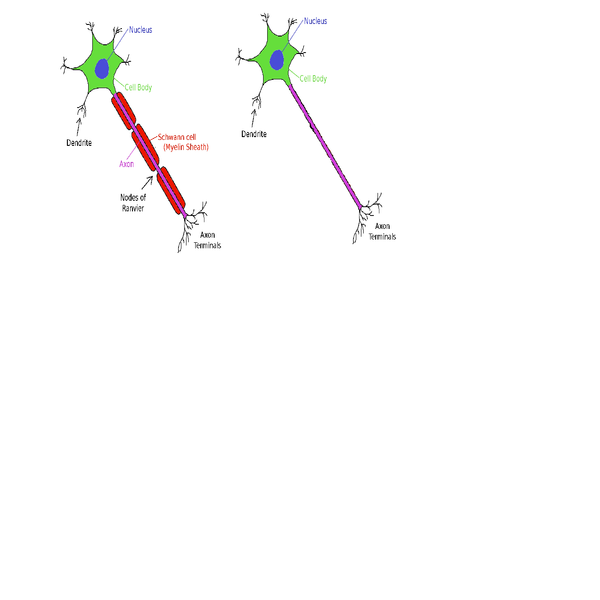
Small fiber neuropathy refers to damage to the small, usually unmyelinated sensory or autonomic nerve fibers running through our skin, peripheral nerves, and organs. These nerves relay sensory information back to the brain and regulate autonomic nervous system functioning.
The symptom presentation is variable–perhaps more variable than doctors know at this point. Nerve-associated symptoms range from feelings of cold, pain, tingling, tearing, buzzing, stabbing, aching, pins and needles, and–what must be a crowd favorite–electric-like shocks lasting several seconds.
Small fiber neuropathy can cause many different types of pain
SFN can also cause the dreaded allodynia or extreme sensitivity to touch. ‘Sensitivity’, though, is hardly the word to describe a condition in which the touch of clothes can feel like sandpaper rubbing against a wound. On the opposite end of the spectrum, some people with SFN can’t feel anything at all.
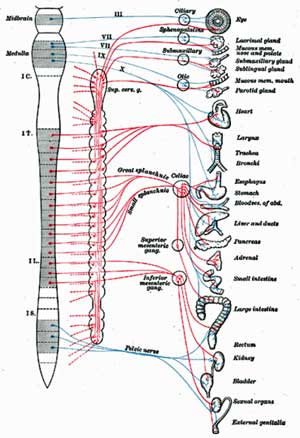
Pain just scratches the surface of the possible symptoms SFN can cause. If the autonomic nerves are involved, dry eyes, dry mouth, lightheadedness upon standing, fainting, abnormal sweating, erectile dysfunction, bladder problems, nausea, vomiting, constipation, difficulty with urinary frequency, etc., can all be present.
The damage–which can extend to outright destruction of the nerves–sometimes first occurs at the ends of the longest nerve fibers in the body such as those found at the tips of the fingers (typically the middle fingers) and the toes, but can take place anywhere the nerves are found.
Quality of life scores, not surprisingly, tended to be on the low side–the very low side.
Diseases Associated with Small Fiber Neuropathy
SFN is associated with a wide variety of diseases and disorders including diabetes, thyroid issues, sarcoidosis, vitamin B12 deficiency, HIV, neurotoxic medications (including chemotherapy and antiretroviral agents), celiac disease, Sjogren’s Syndrome, Lupus. With all these disorders, about 50% of SFN diagnoses are ‘idiopathic’; i.e., no discernible cause is found.
Fibromyalgia
“This provides some of the first objective evidence of a mechanism behind some cases of fibromyalgia, and identifying an underlying cause is the first step towards finding better treatments,” Dr Anne Oaklander
No one had looked at the possible association of SFN with chronic widespread pain or the quintessential pain and fatigue disorder – fibromyalgia - until reports surfaced last year at two conferences two months apart. First Dr. Anne Oaklander, a Harvard neurologist, found high rates of SFN in her young, mostly female (73%) ‘chronic widespread pain’ patients. Their symptom presentation; high rates of autonomic nervous system symptoms (cardiovascular (90%), gastrointestinal (82%), urologic (34%)) plus chronic fatigue (83%) and headaches (63%) suggested they might very easily fit the criteria for fibromyalgia or ME/CFS. Interestingly enough, Oaklander also found many experienced ‘reduced sensation’ (68%) as well as pain.
‘Exhaustive investigations’ which came up zero except for high rates of ‘disordered immunity’ (89%) and a family history of autoimmune disorders (33%) suggested she had an immune disorder on her hands.
Myelinated nerves on the left, unmyelinated nerves on the right. SFN affects the small unmyelinated nerves
Next Oaklander reported at the American Neurological Association (ANA) 137th Annual Meeting in October, 2012, that almost half of the ‘fibromyalgia’ patients in her study (n=54) had evidence of significant small fiber nerve loss, while none of her age and sex matched controls did.
She believed her findings suggested small nerve fiber problems could be driving the central sensitization found in the disorder.
Oaklander then went hunting for evidence of prediabetes/diabetes–a known risk factor for SFN–and found it in a substantial number of patients, most of whom were not aware they had it. (Her study on SFN and FM was published in June of this year.)
Then in a November 2012 conference of the American College of Rheumatology, Dr. Levine of the University of Arizona reported at that 61% of the 56 FM patients in his study had SFN. The burning, stabbing, tingling, allodynia, and autonomic nervous system symptoms often found in fibromyalgia suggested to him that FM patients might have small fiber neuropathy.
(Notice the interesting possible connections to ME/CFS: the autoimmune disorders, the B vitamin deficiency, the diet connection (celiac disease), the pathogen issues, and the neurotoxic connection; virtually every disorder associated with SFN may have some intersection with chronic fatigue syndrome when all is said and done.)
Fibroneuralgia? ME/CFS/FM Doctors Report
Dr. Teitelbaum and Dr. Sivieri are seeing SFN in two distinct sets of ME/CFS/FM patients: an immune set with high rates of dysautonomia (i.e., POTS, neurally mediated hypotension (NMH), and others) but usually less pain, and a pain subset with little dysautonomia. Dr. Teitelbaum emphasized tests are indicating that the majority of patients with fibromyalgia and neuropathic pain are testing positive for SFN.
Dr. Sivieri noted SFN’s ability to affect autonomic nerves across the body suggested that theoretically it could
Sivieri’s been seeing ME/CFS/FM patients for about ten years, and he began digging into IgG subclasses about two years ago. Already using IVIG, his ears pricked up when the SFN results began coming in last year. He felt that nerve problems could help explain why a nerve drug like Lyrica works in some people. With these reports coming in suggesting many FM patients have a nerve (and not a muscle) disorder, he suggests fibromyalgia might be better called ‘fibroneuralgia’. It’s still early yet; he’s just begun looking for SFN in his patients, but he hopes the SFN/IgG connection will help unlock the door to diagnosing what he calls an ‘incredibly elusive’ disease.
Dr. Sivieri believes that if tests show you have SFN in your skin you may very well have it in your gut (gastroparesis-like), bladder and genitals (IC and chronic prostatitis and vulvodynia), central nervous system (POTS), and so on.
Postural Orthostatic Tachycardia Syndrome (POTS)
Although postural orthostatic tachycardia syndrome (POTS) (which is a high pulse rate upon standing) was not on that list, POTS and other forms of orthostatic intolerance should be. Teitelbaum and Sivieri are finding SFN in their POTS patients, and a third of POTS patients in one study had evidence of autonomic neuropathy–damage to the autonomic nerves–and decreased sweat output (suggesting damage to small fiber nerves) was present. The increased rates of headache and gastrointestinal problems found in this group could also be associated with SFN.
In the upcoming blog we’ll look at a POTS patient whose diagnosis with SFN eventually led her to a treatment that worked.
Misdiagnoses are Common
Autonomic symptoms can be misdiagnosed as being due to cardiac arrhythmia, colitis or irritable bowel syndrome, chronic bladder infections, skin allergies, or emotional stress.
As in chronic fatigue syndrome misdiagnoses for small fiber neuropathy are uncommon
Given the varied symptoms SFN can cause, it’s not surprising to learn that, like ME/CFS/FM, misdiagnoses are common. In fact, fibromyalgia is on the list of disorders SFN is sometimes misdiagnosed as. SFN has also been misdiagnosed as multiple sclerosis, regional pain syndrome, fibromyalgia, polymyalgia rheumatica, Raynaud Syndrome, restless leg syndrome, IBS, bladder infections, cardiac arrhythmia, anxiety, and depression.
Causes
Small nerve fibers are rather delicate, unmyelinated nerve fibers which can be impacted by many factors. Diabetes most commonly causes SFN but metabolic, immune-mediated (such as autoimmunity) infections, genetics and other factors can cause it as well.
Many different factors can cause small nerve fiber neuropathy
Increased rates of inflammation, reduced blood flow to the tissues and impaired detoxification processes can whack small nerve fibers. Cytokine upregulation, nerve inflammation and autoantibodies appears to contribute to the SFN found in complex regional pain syndrome (CRPS). Bacterial and viral infections (with a nod towards herpesviruses) can hit small nerve fibers hard. Vitamin deficiencies, with a focus on the B vitamins (B-1,. B-6, B-12), interestingly, given recent suggestions low B-1 may play a role in ME/CFS/FM may be involved, can play a role.
In metabolic syndrome high blood pressure and high levels of cholesterol and triglycerides (present in ME/CFS) contribute. Insulin intolerance whacks the small nerve fibers in prediabetes and diabetes. SFN is common in alcoholism as well.
Immune Connection
Given the accepted treatment (IVIG) it’s not surprising to find immune dysfunctions showing up. Oaklander found high rates of immune dysfunction (primarily reduced C4 levels) and high rates of autoimmunity (33%) in young chronic widespread pain patients.
Dr. Sivieri is finding high rates of low CD57 counts (Stricker Lyme test) and is consistently seeing IgG subclass 1 and 3 deficiencies. A very early study found reduced rates of IgG subclass 1 and 3 in chronic fatigue syndrome. Immunoglobulins or antibodies are proteins produced by B-cells which neutralize pathogens. Reductions in IgG 1 and IgG 3 often occur together and are associated recurrent infections, particularly lung infections.
Low CD57 counts are often associated with Lyme disease, but Dr. Sivieri believes they may be more a marker of chronic infection and immune dysfunction. There’s no doubt that chronic infections can cause nerve damage; the question for him is whether infection gets so strong that it starts taking out the small nerve fibers in our bodies causing dysautonomia and other ME/CFS/FM symptoms.
FM and ME/CFS patients may have low levels of two classes of immunogloblins.
Low levels of IgG subclasses only point to a potential problem, and they need to be tied to recurrent infections for insurance companies to pay for IVIG. IgG subclasses play a big role in the immune system memory that allows it to quickly respond to pathogens that pop up again. IgG tests are often used to determine if you’re battling an infection such as Lyme or chronic mononucleosis, for example.
Dr. Sivieri compares low IgG levels to having a jail without cell doors to keep the criminals (pathogens) in. IgG keeps the pathogens (latent viruses) in their cages and low IgG allows the chronic viruses (HHV6, EBV, HSV) and even bacteria (Lyme, Mycoplasma, etc.) and yeast (Candida) to have their way with the body, joints, guts, and brain, and produce a chronic source of pain, inflammation, and immune dysfunction. Dr. Sivieri believes the low IgG subclasses he sees are a big deal indeed.
You’d be hard-pressed right now to find any fibromyalgia guidelines suggesting that IgG subclass testing be done. Dr. Siveiri reported that most physicians will check total IgG levels only when confronted with sinus or recurrent lung infections, and IgG subclass tests are almost never done. His findings suggest that low IgG subclass levels are much more common in patients with chronic fatigue syndrome and fibromyalgia than normally expected. Beyond that, he can’t say much at this point. Dr. Siveri’s and Dr. Oaklander’s findings suggest that this situation should and will change in the future.
Sivieri has a grant to study the low CD57 count (Stricker Lyme test) and IgG subclass 3 deficiency findings he’s seeing.
Because insurance companies will only pay for IVIG based on low IgG levels AND a history of recurrent infections (i.e., chronic ear, sinus, throat infections and/or frequent colds), Dr. Sivieri emphasized these infections need to be meticulously documented by physicians. Patients should provide a timetable or list of the infections they’ve experienced to their doctors.
Autoimmunity, IgG, and Small Fiber Neuropathy
The autoimmune connection with SFN and low IgG levels is a complicated one. Oaklander did find autoimmunity in about one third of her patients, but she found much more evidence of immune dysfunction. Dr. Sivieri explained that the immune system is so active in autoimmunity that high IgG can sometimes be seen.
Essentially we have at least two immune conditions for creating a small fiber neuropathy: an autoimmune state in which the immune system burns out the nerve fibers, and an immune deficient state in which an infection does the same.
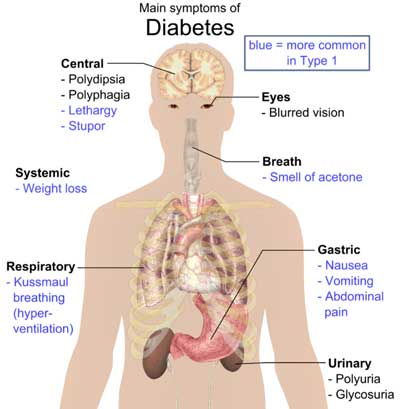
Is There a Diabetes Connection?
I have not found an increase in diabetes in CFS/Fibro patients, but I almost NEVER have seen a CFS/Fibro patient that is not sugar sensitive or doesn’t feel much better when they stop eating sugar in all forms. –Dr. Sivieri
Diabetes can cause SFN and prediabetic states were found in some FM patients with SFN
Oaklander found a significant percentage of patients with diabetes or pre-diabetes in her cohort. Dr. Kogelnik reported that he’s seeing more diabetes than expected in his ME/CFS/FM patients. Dr. Sivieri, however, stated he doesn’t see a lot of diabetes in his patients, but he thinks something is definitely going on with sugar and ME/CFS/FM.
Dr. Sivieri rarely sees ME/CFS/FM patients who are not sugar-sensitive and believes that sugar, insulin sensitivity, and blood sugar dysregulation can play a large role in these disorders. In fact, he questioned whether any patient consuming a lot of sugar products could ever make a substantial recovery.
He believes it goes further than blood sugar; sugar contributes to the almost universal gut dysbiosis he sees in these disorders. Another good reason to get off sugar (in all its forms (sigh)) is that high blood sugar levels can also permanently damage the very nerves we’re talking about.
Treatment
“These findings suggest that some patients with chronic pain labeled as fibromyalgia have unrecognized SFPN, a distinct disease that can be tested for objectively and sometimes treated definitively,” Dr. Anne Oaklander
Levine was able to find a treatable cause for the SFN in about two-thirds of those testing positive for SFN. Problems with glucose metabolism led the list (n=11), with a significant percentage having vitamin D deficiency (n=5), two having Sjogren’s syndrome, and two with elevated erythrocyte sedimentation rates.
Oaklander reported high ‘improvement’ rates using IVIG in a small study (15 patients). Dr. Sivieri, however, is not finding IVIG to be a useful standalone treatment for fibromyalgia/CFS, particularly in patients who’ve had the disorder(s) for some time. Too much has gone wrong and too much (sleep, diet, pituitary function, brain chemistry) needs to be addressed for IVIG to be a cure-all in his patients. IVIG appears to be working best in ME/CFS/FM patients with low IgG subclasses.
A drug in clinical trials called ARA 20 designed to activate repair mechanisms and reduce inflammation showed some promise in sarcoidosis patients with SFN.
Both Dr. Teitelbaum and Dr. Sivieri emphasized, however, that we’re in early days of learning about the connections between SFN, IgG subclasses, treatment effectiveness, and ME/CFS/FM. Both are investigating the SFN connection in their patients now, and we should know much more by the end of the year.
At a chronic pain conference Dr. Daniel Clauw noted how surprised pain researchers were at the role the immune system plays in producing pain. With several positive FM immune studies recently, a prospective FM diagnostic test based on immune findings, and now this rapidly emerging evidence of an immune mediated nerve problem in FM/ME/CFS, it’s a good bet researchers are going to give the immune system in FM a deeper look. It’s not surprising that he has to start the IVIG lower than recommended and then carefully calibrate the dose with each individual patient. Most insurance companies, however, balk at paying for IVIG more than once every three to four weeks.
Diagnostic Tests
QSART (Quantitative Sudomotor Axon Reflex Test)
An autonomic nervous system test called QSART is most commonly used to diagnose SFN, although it’s more a measure of autonomic functioning than nerve damage. Sivieri does not believe results of QSART tests will be enough to get insurance companies to pay for IVIG.
Therapath
Dr. Sivieri uses a diagnostic services company named Therapath (www.therapath.com) which he described as being very professional and easy to work with.
Video -
The test kits Therapath mails to the doctor need to be refrigerated and have a limited shelf life. They come with tweezers, scissors, the skin punch device, etc., and Therapath provides a teaching video on their website. A 3-mm dermatologic punch is used to extract small skin cores that are examined for nerve fiber density. According to the scientific literature, the sensitivity (78%–92%) and specificity (65%–90%) of skin biopsy tests are good. The biopsy is very small and leaves a very small scar.
Because Therapath has control data for only three locations on the legs, the biopsies must be done in those areas for pathologists to certify a positive test. It is interesting that the biopsies are not done in areas where people with fibromyalgia feel much pain.
Insurance companies usually pay a significant portion of the costs.
Conclusions
“The next step of independent confirmation of our findings from other laboratories is already happening, and we also need to follow those patients who didn’t meet SFPN criteria to see if we can find other causes. Helping any of these people receive definitive diagnoses and better treatment would be a great accomplishment.” Dr. Anne Oaklander
It’s very early yet but small fiber neuropathy has the potential to present an entirely new way of looking at fibromyalgia and chronic fatigue syndrome. Well accepted and easily diagnosable, (at least in the skin), SFN may present a new pathway to legitimization for both these disorders. With the possibility that multiple system involvement could produce a wide range of pain and autonomic symptoms, SFN could be made to order for symptom-rich disorders such as ME/CFS and FM.
Dr. Oaklander cited high success rates with IVIG that may or may not translate to ME/CFS or FM. Citing expense, Dr. Teitelbaum has eschewed IVIG, for years but now holds out hope it may help his more severely ill patients. With some miracle cures and mostly moderate results, Dr. Sivieri sees IVIG as one tool that needs to be supplemented with others to be successful.
With just one published study, two conference reports and a host of anecdotal findings we’re still very early in the SFN saga. The next year will tell us much.
(Thanks to Dr. Teitelbaum and Dr. Sivieri for their help. All errors are mine)